Hip Fracture Treatment
Intertrochanteric Fracture, Subtrochanteric Fracture, Subcapital Fracture, Femoral Head Fracture, Greater Trochanter Fracture
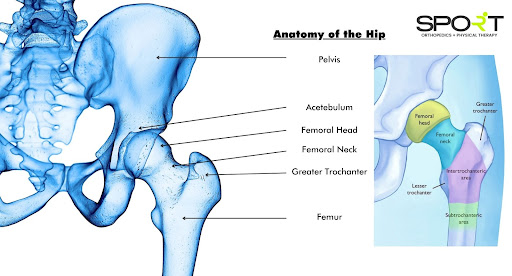
Hip Anatomy
The hip can be described as a ball-and-socket joint. The head of the femur, which is the top section of the thigh bone, is the ball. The acetabulum is the name for the socket and is a part of the pelvis. A rounded shape surrounds the femoral head.
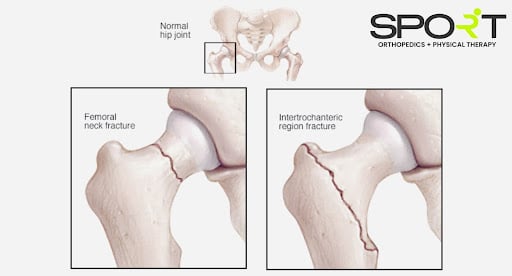
The most popular forms of hip fractures are intertrochanteric and femoral neck fractures. Femoral head fractures are highly uncommon, and these fractures occur as a byproduct of high-velocity trauma.
One of four regions of the upper femur can incur an injured hip fracture:
- Femoral neck: The femur’s portion below the ball (femoral head).
- Intertrochanteric area: The space between the femur’s neck and the bone’s central section, or shaft. The greater and lesser trochanters are two bony markers that distinguish it as intertrochanteric.
- Subtrochanteric area: The upper portion of the femur shaft beneath the greater and lesser trochanters.
- Femoral head: The femoral ball that is seated in the socket.
What Causes a Hip Fracture?
Low-energy falls in older people with fragile or osteoporotic bones cause the majority of hip fractures. Even a little twisting or tripping accident might result in a fracture in these individuals.
The bone might be so fragile that the fracture arises randomly while walking or standing for some. “The break comes before the fall,” as the phrase goes in this context. Femoral neck fractures are the most common for sudden fractures.
Stress fractures or fractures due to repetitive collision are possible in the femoral neck. Long-distance athletes, notably military recruits in initial training, are prone to these fractures. Stress fractures in the subtrochanteric area of the hip are frequently linked to the use of specific osteoporosis drugs for a long time.
Femoral head fractures are uncommon and generally happen due to a high-impact accident or a hip fracture dislocation.
Hip Fracture Diagnosis
A femoral neck fracture or the intertrochanteric area break is by far the most common site for hip fractures. The fracture’s placement contributes to determining the best treatment recommendations.
Symptoms and the incorrect posture of your hip and leg can sometimes lead to a hip fracture diagnosis. An X-ray will typically prove the existence of a fracture and reveal the location of the fracture.
If your X-ray shows no breakage but hip discomfort remains, the doctor may conduct an MRI or a bone scan to check for a fracture like a hairline or microscopic.
Typically hip fractures form in two places on the long bone (femur) that connects your pelvis to your knee: the femoral neck or intertrochanteric region.
What Are Symptoms of a Hip Fracture?
A hip fracture is usually excruciatingly painful. The crotch and top region of the thigh are frequently the sites of discomfort. Often these hip fractures prevent you from standing, bearing weight, or moving the upper half of your leg or knee. Unless you have an ailment to your lower leg in combination with the hip, you should be capable of trying to move your ankle and toes.
Certain fractures might allow for some pressure to be placed on your leg, although this will be extremely uncomfortable.
Treatment Options for a Hip Fracture
Metal screws, plates, and rods can fix a hip fracture. Artificial substitutes (prostheses) of sections of the hip joint may be required under certain circumstances.
The most common treatment for a hip fracture is a mix of surgery, rehab therapy, and prescriptions.
To further elaborate, most hip fractures require surgery within 1 to 2 days following the accident. Only a tiny percentage of nondisplaced fractures in healthy people can be managed short of surgery. Another minority of patients could be too unwell to undergo surgery without considerable risk.
Surgical treatment is essential to ease the acute suffering caused by a fracture, enabling the individual to get up from the bed. It is feasible to reduce the risk of problems by undergoing surgery promptly.
An internist and preoperative screening may be conducted if you are brought to a hospital with a hip fracture concern. This internist will inspect you for your surgery eligibility and risk. To address specific medical conditions, you should consult a specialist, such as a cardiologist or a pulmonologist. You should wait on clotting improvement before surgery if you have been on blood-thinning medications.
The term “optimization” refers to the process of medically preparing a subject for surgery. It must be completed within 48 hours, but rare cases could take more time. Even though it could drag on longer than expected, being optimal is preferable to rushing into a surgery.
The nature and placement of different types of hip fractures, including the patient’s age and health, all influence treatment options.
Hip Fracture Surgery
The surgical treatment you receive is usually determined by the location and severity of the breakage if the shattered pieces are misaligned (aka displaced) and your age and underlying health issues. Among the possibilities are:
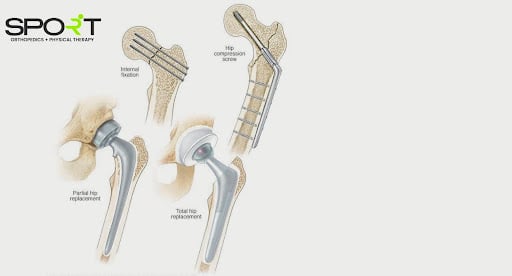
- Internal repair using screws: Screw fixation is used to restore the inside. Solid and durable, stainless steel and titanium screws are placed into the fractured bone to keep it together for the healing duration. Sometimes, there will be a metal plate for screw fixation stability along the femur.
- Partial hip replacement: A surgeon may extract the head and femoral neck bone and implant a metal prosthetic if the end(s) of the shattered bone is displaced or destroyed. Those with additional health problems, cognitive disability, or inability to live independently may benefit from a partial hip replacement.
- Total hip replacement: Manufactured pieces substitute the upper femur and the socket in your pelvic bone (prostheses). Research demonstrates that complete hip replacement seems more cost-effective/affordable among apparently robust independent adults and is linked with superior long-term results.
If the blood supply circulating to the ball component of your hip joint has been injured from the fracture, your doctor may propose a partial or complete hip replacement. The bone is much less certain to mend adequately in this type of injury, most common in elderly adults with femoral neck fractures. Below is a better understanding of each type of hip fracture that is common.
Femoral Neck Fractures
A subcapital or intracapsular fracture is another name for this specific type of fracture.
In-situ pinning is the most common treatment for femoral neck fractures which isn’t displaced. Surgical pins and screws will be placed through the fracture site to prevent the femur’s ball from moving throughout the healing process. The femoral head is pinned to prevent dislodging or falling off the femoral neck, requiring hip substitution.
Femoral neck fractures can be repaired sans surgery in a limited percentage of cases. Non-displaced fractures are more common among younger, robust individuals. Still, they will need to be closely watched as displacement is possible. Nonoperative therapy consists of reduced or shielded pressure carrying crutches for a few weeks.
Nonsurgical therapy could be explored for people who could not walk before surgery or those who have serious medical conditions.
Displaced femoral neck fractures are more intensive to treat than nondisplaced fractures. The posterior capsule is a framework that supplies blood circulation to the femoral head. Because a displaced femoral neck fracture frequently injures the posterior capsule, the break has far less possibility of healing.
Regardless of if the breakage heals, the femoral head could become diseased with avascular necrosis. That can further result in bone cell destruction, the loss of a portion of the head of the femur, and eventually develop arthritis.
As a result, displaced femoral neck fractures are frequently addressed by hip replacing. Hemi-arthroplasty, aka partial hip replacement, is the preferred option for the elderly. Complete hip replacement would be recommended for younger, more active individuals.
It is preferable to keep the native femoral head in certain younger individuals instead of replacing it. An open reduction is performed on such individuals. This procedure entails creating an incision above the hip joint, repositioning the bone, and securing it with pins, screws, or other metal fixation. Although there is a danger of avascular necrosis and failure to heal with this treatment, it is thought that it is preferable to keep a younger person’s natural hip.
An orthopedic surgeon will discuss your treatment choices and more suitable options.
Intertrochanteric Femur Fracture
Intertrochanteric injuries arise in the broader area between the greater and lesser trochanter, underneath the femoral neck. The greater trochanter is the bulge on the side of your hip that you can feel. Two, three, or even more fracture pieces are possible.
These two-part part fractures (left) or three-part (right) are repaired surgically with compression sliding hip screws and side plate or an intramedullary nail.
Bone screws secure the compression sliding hip screws to the exterior surface of the bone. A lag screw, aka a large secondary screw, is inserted into the head and neck of the femur via the plate. This design makes the impaction and compression at the injury site possible. This will aid recovery and boost fracture stability.
A compression sliding hip screw and a side plate treated a two-part intertrochanteric fracture. The intramedullary nail is usually inserted into the bone’s marrow canal through an incision at the top of the greater trochanter. After that, several screws are driven through the nail then into the femoral head.
An intramedullary nail would be used to repair a two-part intertrochanteric hip fracture.
Fracture of the Greater Trochanter
A minimal impact domestic fall is the most common cause of isolated greater trochanter fractures. Even though they are frequently painful, they usually recover without the need for surgery. These breaks are stabilized and managed using crutches or even a walker.
An MRI is typically recommended when an x-ray reveals an independent greater trochanter break to ensure that the fracture does not spread to the intertrochanteric region.
Subtrochanteric Fracture
The top section of the femur shaft, right behind the hip joint, is affected by subtrochanteric fractures.
These are surgically repaired by inserting an intramedullary nail into the femoral neck and a screw into the femoral head through the nail.
More screws might be put at the lower end of the nail at the knee to prevent the nail from rotating or shortening (telescoping) on the nail. Interlocking screws are what they’re called.
Rather than a nail, your operator could opt for a compression sliding hip screw with a lengthy side plate in rare circumstances.
Femoral Head Fracture
Femoral head breaks are uncommon; only around 1% of all hip fractures are femoral head fractures. They are frequently the outcome of a high-velocity incident. There is a chance that the hip joint socket will be fractured.
Nonsurgical treatment with minimal weight-bearing is possible if it is not displaced. If the displaced fragment is minor and does not cover a considerable portion of the joint surface, it can be easily removed.
When a big fragment is present in active and younger patients, open reduction and screw fixation is frequently used. Hip restoration, partial or complete, to substitute the compromised femoral head is the preferred treatment for elderly patients.
What Is Recovery Like for Hip Fractures?

Most people can get out of bed the day following surgery and begin physical rehab. It’s critical to get started ASAP. Medical issues like blood clots, pneumonia, or bedsores are less likely due to this. This even aids in the prevention of disorientation and deconditioning in elderly patients.
In the elderly, hip fractures can result in disability and loss of independence. Long-term outcomes have been demonstrated to be improved by early mobility and rehabilitation.
Physical and occupational therapists will help you throughout your recovery. They will offer you workouts and advise you on how much weight you can bear on your leg/hip. They will also demonstrate what to do to perform everyday routines, including bathing and dressing.
Postoperative Care
Those who have had surgery generally require a walker, crutches, or perhaps a wheelchair. The patient’s doctor would usually advise them to burden the fractured hip as they are comfortable with it as it heals. Physical treatment will very certainly be required. You might have to stay in a rehab or treatment center until you become well enough to return home, though it is dependent on your living arrangement. When a patient’s leg is mended, a doctor may advise them not to put any pressure on it. This is a per case and per person decision, and your doctor can explain why this might be essential.
It is critical not to only stay in bed following a procedure merely. You should sit up frequently throughout the day. It will help prevent pneumonia, bedsores, and blood clots and encourage you to use your leg more often. It’s imperative to proceed with caution. Nurses, relatives, physical therapy, or the use of a walker or cane might be necessary.
Rehabilitation
On the first day following surgery, your treatment team will most likely urge you to get out of bed and move. The first priority of physical therapy will be on range-of-motion and strength activities. You may have to transfer to a prolonged care facility due to the sort of operation you had and if you have support at home.
You may engage with an occupational therapist in long-term treatment or at home to acquire strategies for everyday freedom such as toileting, bathing, dressing, and cooking. A walker or wheelchair may be recommended to help you recover mobility and function.
Complication of Hip Fractures
Given a distinctive abnormality at the fracture site, the most common complication following treatment is a varus and procurvatum malunion or nonunion. This problem can be reduced by establishing an appropriate reduction and stable fixation at the time of first operation. It’s vital to screen out any systemic factors to the nonunion, including vitamin or mineral deficits, as well as infection, as should be with all fracture nonunions. After systemic causes have been eliminated or treated, revisions can begin with the goal of rectifying the abnormality.
Long Term Expectations

Patients may limp postoperatively on occasion. This could become better or disappear with physical therapy. Your hip may become more fatigued or stiff than it was prior to the procedure. It’s infrequent, but plate, rod, or screws might cause patient hip pain. In specific circumstances, the bone may not mend if there is a problem like an infection develops. An additional operation could be required if this occurs. Even if your operation is successful, you may need to rely on a walker or cane all of the time. Even if you have never used one previously, this could still happen. The essential thing is to avoid falling again. A walker or cane can help you to keep your balance and prevent you from falling again.
What to Expect from Your Doctor’s Visit
A doctor may ask a few questions, such as:
- Have you suffered recently from a fall or hip injury?
- What is the severity of your hip pain?
- Is it possible for you to put any pressure on the leg on the affected hip?
- Have you undergone a bone density examination?
- Have you ever been told you have some other health issue(s)? What drugs, including vitamins and supplements, are you presently taking?
- Do you consume alcoholic beverages or smoke cigarettes?
- If you’ve ever had surgery on your body? If there were any difficulties?
- Do you have any family members with a past of bone fractures or osteoporosis, including a parent or sibling?
- Do you live alone?
Contact SPORT Orthopedics and Physical Therapy Today
At SPORT, we pride ourselves on offering only the best in orthopedic surgery and physical therapy in Dallas. Our Dallas orthopedic surgeons have extensive experience treating injuries through both surgical and nonsurgical means. If you need fracture surgery, hip arthroscopy, hip labral tear surgery, hip replacement, or hip resurfacing, we’ve got you covered. To schedule an appointment with a provider, please call 469-200-2832 or fill out our online intake form.










































")


